

Background
Double induction using two subsequent 7+3 regimens of cytarabine plus anthracycline is commonly performed in AML patients with an adequate performance status in order to maximize dose intensity upfront. However, for patients with a good early response at day 15 of first induction, there is no prospective randomized evidence on the necessity or value of a second induction cycle.
Aims
In order to answer the question if good responders of the first 7+3 induction could be spared a second induction cycle, we set up randomized-controlled SAL DaunoDouble trial. The study prospectively assesses the outcome of patients with a good early response with respect to the number of induction cycles (single versus double). We assumed non-inferiority of single induction in terms of complete remission (CR/CRi) rate, based on a margin of 7.5%. Here, we present the results of the planned interim analysis.
Methods
Patients (pts) 18-65 years with newly diagnosed AML, normal cardiac and organ function received a first induction cycle with seven days of cytarabine plus three days of daunorubicin ("7+3"). Response assessment in bone marrow was done on day 15 after the initiation of chemotherapy and confirmed by central review. A blast count <5% was defined as good response. Pts with good response were randomized to receive a second induction cycle (arm D) or no second induction cycle (arm S). Primary endpoint was CR/CRi after completion of induction, secondary endpoints were RFS, and OS.
Results
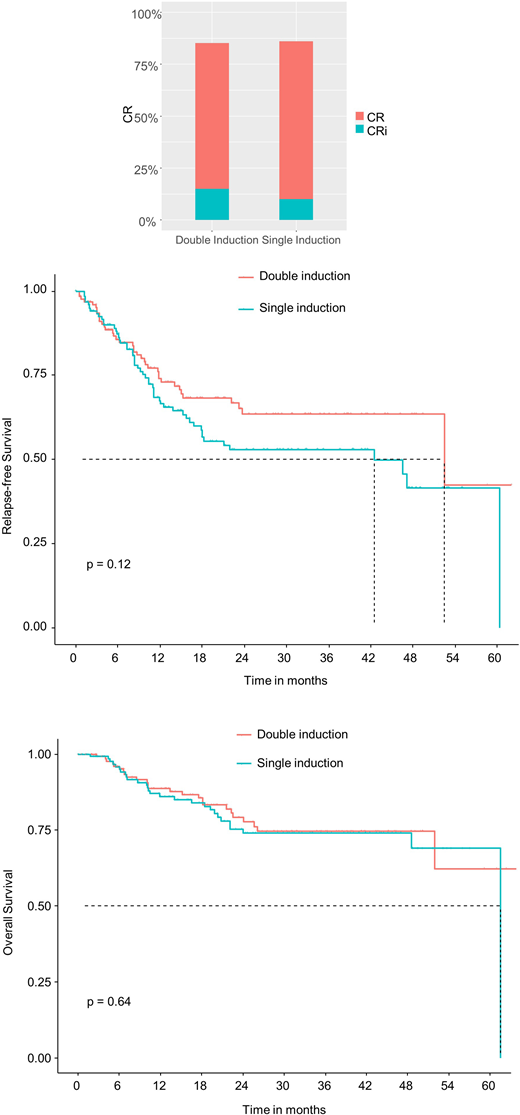
Between 2014 and 2020, 624 evaluable pts were enrolled and received the first induction cycle with 7+3. A marrow blast clearance below 5% on day 15 was achieved in 298 pts (48%), providing eligibility for randomization. Of these patients, 150 were randomized into arm S and 148 into arm D, respectively. Median age was 52 years, 92% had de novo AML, NPM1 mutation was present in 53%, FLT3-ITD in 25% of pts. Favorable, intermediate and adverse risk (ELN 2017) were present in 56%, 34% and 10% of pts, respectively. CR/CRi rates at the end of induction were 86% after single induction and 85% after double induction. The CR/CRi rates in 224 pre-defined per-protocol pts were 88% versus 91%, resulting in a CR difference of 3% (95%-CI -0.047-0.111; p for non-inferiority test 0.145). After a median follow-up time of 24 months, RFS was slightly but not significantly lower after single induction with a 3-year RFS of 53% versus 64% (HR 1.4, p=0.125), whereas no differences were seen in 3-year OS, with a of rate of 74% versus 75% (HR 1.1, p=0.645) after single versus double induction.
Conclusion
The interim analysis results show that in good responders, the difference between CR rates after single versus double induction was even smaller than the predefined 7.5% margin, suggesting a trend for non-inferiority of single induction, although statistical significance was not reached. The trial continued recruitment. These findings suggest that in good responders, it may be safe to omit a second induction cycle if a second cycle poses a high risk.
Figure. CR + CRi, RFS and OS after randomization to single versus double induction.
Alakel:Pfizer: Consultancy. Jost:Pfizer: Membership on an entity's Board of Directors or advisory committees; Astellas: Membership on an entity's Board of Directors or advisory committees; Roche: Membership on an entity's Board of Directors or advisory committees; JAZZ: Other: travel support; Celgene: Other: travel support. Novak:Roche: Consultancy; Janssen: Other: Travel expenses; Takeda: Consultancy; Amgen: Consultancy, Other: Travel expenses; Pfizer: Consultancy; Novartis: Consultancy. Krause:Takeda: Honoraria; Celgene: Other: Travel Support; MSD: Honoraria; Pfizer: Honoraria; Siemens: Research Funding; Gilead: Other: Travel Support. Held:Roche: Consultancy, Other: Travel, Accommodations, Expenses, Research Funding; BMS: Consultancy, Other: Travel, Accommodations, Expenses, Research Funding; MSD: Consultancy; Acrotech: Research Funding; Spectrum: Research Funding; Amgen: Research Funding. Platzbecker:AbbVie: Consultancy, Honoraria; Amgen: Honoraria, Research Funding; Geron: Consultancy, Honoraria; Takeda: Consultancy, Honoraria; Janssen: Consultancy, Honoraria, Research Funding; Novartis: Consultancy, Honoraria, Research Funding; BMS: Consultancy, Honoraria. Thiede:AgenDix GmbH: Other: Co-owner and CEO. Müller-Tidow:Daiichi Sankyo: Research Funding; Pfizer: Research Funding, Speakers Bureau; BiolineRx: Research Funding; Janssen-Cilag GmbH: Speakers Bureau.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal